You need to see a rheumatologist if you suffer from pain, swelling, and limited joint function. What happens when all your laboratory tests are negative or “so called” normal? Some of you will get a diagnosis of seronegative rheumatoid arthritis.
In this article, I will discuss the most critical aspects of a seronegative rheumatoid arthritis diagnosis and answer the following questions.
-
- What is Seronegative Rheumatoid arthritis?
- Can seronegative RA mimic other types of arthritis?
- Is seronegative RA more aggressive than seropositive RA?
- Can seronegative RA become seropositive? and
- Is the treatment different for seronegative RA?
What is Seronegative Rheumatoid arthritis?
I think it is essential to understand that rheumatoid arthritis is the most common autoimmune disease that I, as a rheumatologist, see and diagnose in my clinic. Rheumatoid arthritis (RA) affects approximately 1.5 million people in the US. Females are more affected than men.
Diagnosis of rheumatoid arthritis
Before we make the diagnosis of rheumatoid arthritis, we pay attention to the clinical picture. The classical pattern of RA involves pain and swelling in the joints, especially the hands and feet, in a symmetric and bilateral pattern. So, hands, feet, shoulders, knees, and ankles are affected simultaneously. Morning stiffness is also characteristic and usually lasts more than one hour and is improved by movement. Here is a video about the most common five signs and symptoms of rheumatoid arthritis.
Then, to help with our diagnosis, we order labs and X-rays. We commonly order laboratory tests for patients where we suspect RA are Rheumatoid factor and Anti-CCP antibodies (anti-cyclic citrullinated peptide antibodies), along with other labs that I will discuss in another article.

Now, when researchers have looked at percentages of patients with positive markers, they have found that only
60-80% have positive Rheumatoid factor
65% have anti-CCP antibodies
And
About 20% of rheumatoid arthritis cases have none of these markers positive.
If those markers are positive, or only one is positive in the patient’s serum or blood, I diagnose patients with seropositive rheumatoid arthritis. If those markers are negative, I will diagnose patients with seronegative RA, meaning the patient’s blood/ serum does not contain positive RF and anti-CCP antibodies.
To make things more complicated, none of these markers make a diagnosis of rheumatoid arthritis. These markers should be used in conjunction with the clinical picture, the onset of the symptoms, and, sometimes, elevated markers of inflammation.
At times, the diagnosis of seronegative RA can be delayed due to negative markers, leading to a more advanced and destructive disease.
Can seronegative RA turn into other types of arthritis?
The short answer is YES. Seronegative RA can turn into another type of arthritis. A recent study published in 2021 proved that many patients initially diagnosed with seronegative RA developed other forms of arthritis in the next few years.
From 9700 patients initially diagnosed with seronegative RA, approximately 560 changed their diagnosis.
Of these 560 patients, about 48% had Psoriatic arthritis, 43% had axial spondyloarthropathy, and the rest had inflammatory bowel disease arthritis.
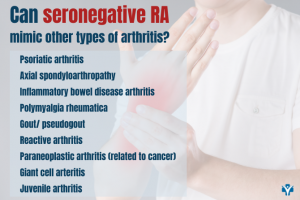
Some situations of Sjogren Syndrome or Lupus patients can present with signs and symptoms of seronegative RA, so I recommend obtaining at least an ANA test in the initial battery of autoimmune testing for new-onset patients.
In 2019, another study also identified other causes of seronegative RA like
- polymyalgia rheumatica
- gout/ pseudogout
- reactive arthritis
- paraneoplastic arthritis (related to cancer)
- giant cell arteritis
- juvenile arthritis
This is quite common in rheumatology, as autoimmune diseases develop and evolve over many years.
In my practice, I have diagnosed many patients with seronegative RA that eventually developed psoriatic arthritis in my practice. To learn more about psoriatic arthritis check my video about the most common signs and symptoms of psoriatic arthritis.
If you are a patient with psoriasis, even many years ago, tell your doctor about that. If you are a patient that has a history of Crohn’s or Ulcerative colitis, also mention these to your rheumatologist if you are not asked. If you also have lower back pain, frequent tendonitis like Achilles tendonitis, elbow tendonitis or even inflammatory disease of your eyes, mention these as they could be signs of axial spondyloarthropathy or ankylosing spondylitis.
Is seronegative RA more aggressive than seropositive RA?
There is an ongoing debate. The truth is that we still do not know. In seropositive RA patients, certain risk factors such as anti-CCP antibodies, are associated with poor prognosis or more aggressive disease. However, early diagnosis and aggressive treatment in the early stages of the disease can potentially stop the inflammation and prevent further damage of your joints. Being proactive and under the care of a specialist physician will help you to manage the disease better.
Can seronegative arthritis become seropositive?
Yes, some patients can become positive in time, although we are not sure at this time what percentage of patients will become seropositive.
Is routine testing recommended? Not really, but in certain situations, your rheumatologist will decide to retest you to make sure you did not develop another type of autoimmune disease.
Is the treatment different for seronegative RA?
Once a diagnosis of seronegative RA is made, your rheumatologist will discuss your therapy options. The treatment is not different from seropositive rheumatoid arthritis, but it will need to be individualized to your medical situation. As a general rule, the RA treatment is done in a step-wise approach, starting with the least aggressive medications such as non-steroidal anti-inflammatory medications and hydroxychloroquine, then advancing to other disease-modifying anti-rheumatic drugs like leflunomide, methotrexate or sulfasalazine.
More targeted therapy is indicated if those drugs are ineffective or not tolerated.
These medications are collectively named “biologics”. If you want to learn more about biologics, watch this video on my channel.
Biologics is a general term for many medications targeting molecules that produce inflammation in your body, like TNF-alpha, IL-6 or JAK enzymes. For treatment recommendations, you should discuss in depth your clinical situation with a rheumatologist that will be able to answer specific questions.
Diagnosis of seronegative RA can be problematic in the absence of positive markers. The clinical picture is extremely essential in evaluating a patient with arthritis. As a rheumatologist, I listen to the patient and thoroughly analyze the pattern of the disease. This allows me to diagnose and treat patients earlier and more appropriately. If you are looking for a consultation for arthritis or autoimmune disease, schedule on our website Rheumatologist OnCall. I am happy to evaluate and treat you with the most comprehensive and personalized approach that will integrate the most cutting-edge science with integrative medicine, which includes nutrition, supplements, stress management, mindfulness, exercise, and sleep management.